Updated and contextualized version of an article originally published on June 19, 2014
The article retains its original focus by presenting it through a scholarly and accessible perspective, supported by verifiable references.
Authors
- Dr. A. Colonnese – Nutrition biologist
- Roberto Panzironi –Independent researcher
Note editoriali
- First publication: June 19, 2014
- Last update: April 18, 2026
- Version: 2026 narrative revision
Initial Note: This article was previously published and has been updated according to scientific and informative criteria. It is for informational purposes only and does not replace personalized medical advice. For health decisions, consult your doctor.
IN BRIEF
- Literature suggests associations between diets with a high glycemic load/index, high consumption of sugary drinks, and worse outcomes for certain cancers, particularly colon cancer in the post-diagnosis stage.
- Plausible mechanisms include hyperinsulinemia, activation of the IGF (insulin-like growth factor) axis, and metabolic alterations that promote cell proliferation; however, causal evidence in humans remains incomplete.
- Experimental studies in animal models show that diets rich in sugars or that induce hyperinsulinemia can accelerate tumor growth; results are not automatically transferable to humans.
- Among the cancers studied, the most robust evidence regarding the post-diagnosis relationship concerns colon cancer recurrence in some subgroups.
Abstract: what does science say?
Topic: the possible relationship between excessive consumption of sugars/high glycemic index carbohydrates and the development, progression, or recurrence of cancer. The evidence is heterogeneous: observational studies on populations and cancer survivors indicate associations between insulinemic diets (high glycemic load, sugary drinks) and worse outcomes for some cancers; experimental studies in animal models show that diets that elevate insulin or glucose can promote tumor growth. However, definitive causal evidence in humans is lacking for most cancers: results depend on dose, carbohydrate quality, glycemic index, metabolic status (e.g., overweight/obesity, insulin resistance), timing (before vs. after diagnosis), and exposure measurement. Limitations include dietary assessment errors, confounding by lifestyle, and tumor heterogeneity. In summary, biological plausibility exists, and consistent epidemiological signals are present in specific contexts, but interpretation requires caution.
What clinical and epidemiological evidence shows
In observational studies and cohorts of cancer patients, certain dietary patterns characterized by a high glycemic load or frequent consumption of sugary drinks have been associated with a higher risk of recurrence and mortality in specific contexts. For example, among patients with stage III colon carcinoma, prospective studies linked to the large CALGB 89803 trial showed that dietary scores with high insulinemic potential or a high glycemic load after surgery were associated with worse clinical outcomes in subgroups of patients; similarly, frequent consumption of sugary drinks was linked to a higher risk of recurrence in that cohort. [1] [2] [3]
Cohort studies on general populations report mixed results: some analyses of Mediterranean and European populations (e.g., EPIC-Italy) have shown an association between high glycemic index or load and an increased risk for colorectal and other site cancers; other meta-analyses show modest or absent associations depending on the type of study, the quality of dietary measurement, and control for confounding factors such as body weight and physical activity. [8]
Epidemiological Interpretation
These data are observational: they show correlations that may be consistent with a biological effect of hyperinsulinemia on cancer, but they do not automatically prove that increasing sugar in the diet causes cancer. The association may depend on dose (how much sugar), frequency (how often), carbohydrate quality (glycemic index), individual metabolic status (obesity, insulin resistance), and timing relative to diagnosis. Individuals with overweight/obesity and insulin resistance appear to be more vulnerable to the adverse effects of diets with high insulinemic potential. [8] [6]
Plausible biological mechanisms
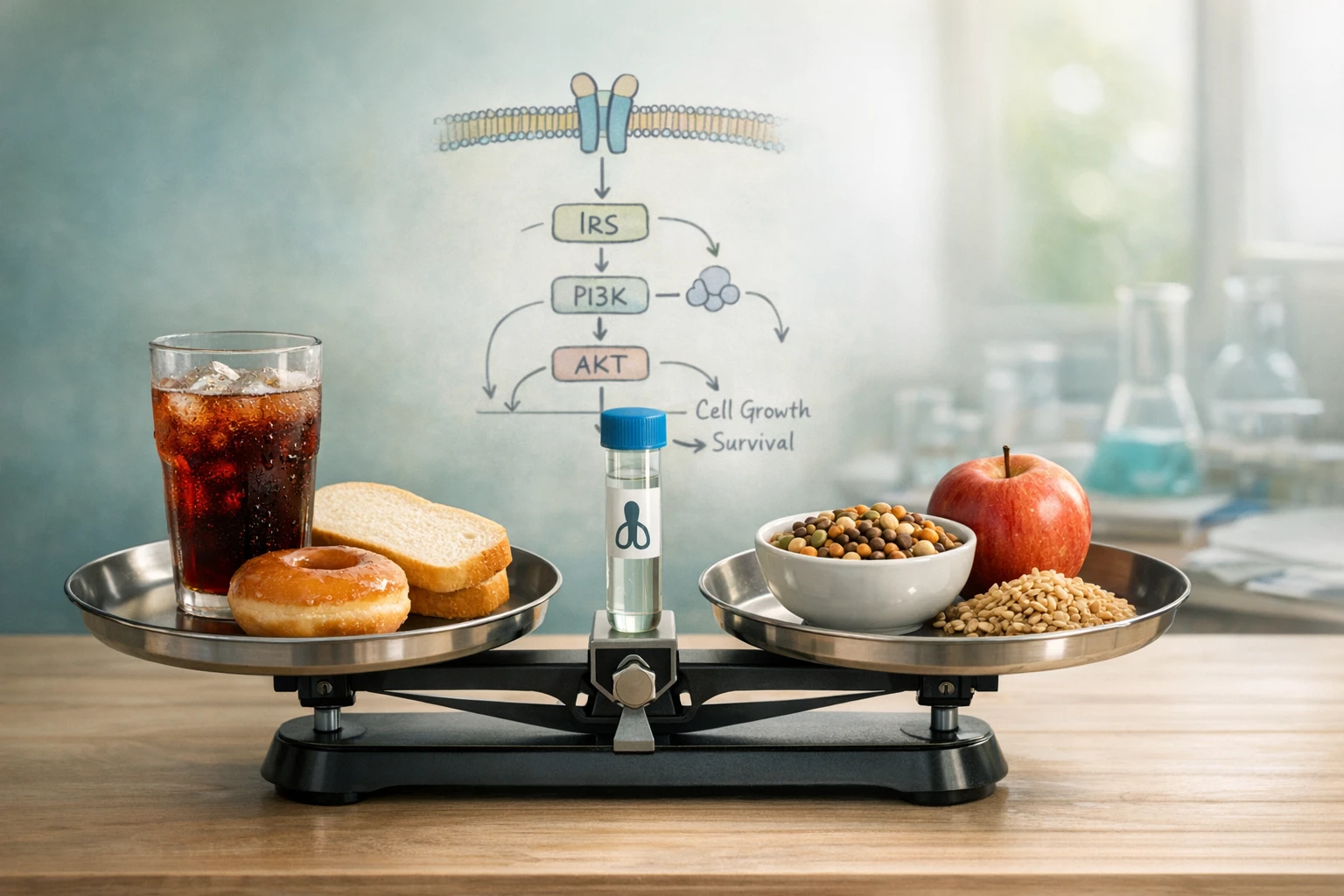
The biological plausibility linking sugars/high glycemic index carbohydrates and cancer is mainly based on two lines: 1) the insulin/IGF axis and 2) the availability of metabolic substrates. The hypothesis is that elevated postprandial glycemic peaks induce insulin secretion; chronic hyperinsulinemia can increase mitogenic signaling through the insulin and IGF receptors, supporting cell proliferation and survival, and reducing apoptosis. [6] [7]
Furthermore, a high glucose environment can promote cellular metabolic reprogramming processes (e.g., increased aerobic glycolysis, known as the Warburg effect), providing energy and precursors for the synthesis necessary for tumor proliferation. Finally, altered metabolism and inflamed adipose tissue generate cytokines, adipokines, and oxidative stress that modulate the tumor microenvironment and the risk of progression. These mechanisms have been discussed in recent reviews and supported by experimental data. [6] [7]
Limitations of mechanistic plausibility
Not all tumors express the same receptors or respond equally to insulin/IGF; moreover, clinical measures of insulin and glucose are often variable and influenced by other factors (medications, oncological therapy, overall diet). Therefore, the biological heterogeneity of tumors requires caution in translating mechanisms into generalized clinical recommendations. [6]
Experimental evidence and data from animal models
In animal models, numerous experimental studies have shown that diets rich in sugars or that induce hyperinsulinemia can increase the incidence or growth of tumors in organs such as the liver and prostate. For example, in murine models of hepatocarcinogenesis, a sugar-rich diet increased tumor incidence compared to low-sugar diets. [5]
Similarly, xenograft models of prostate carcinoma have shown accelerated tumor growth in mice fed diets high in refined carbohydrates, associated with increases in insulin and IGF-1; in some experiments, reducing carbohydrate intake slowed tumor growth. [4] These results strengthen the hypothetical mechanism of hyperinsulinemia → tumor promotion, but direct transposition to humans is complex due to metabolic differences, dosages, and experimental conditions.
What it means in practice
For the general public: data indicate that chronic excess of simple sugars and diets with a high glycemic load can contribute to a metabolic state (hyperinsulinemia, insulin resistance, obesity) that is associated with an increased risk and worse outcomes for some forms of cancer. This does not mean that sugar is the sole or direct cause of cancer for every individual, but that controlling metabolic status is relevant for general health and, in cancer patients, can influence the course of the disease.
Non-prescriptive practical indications: favoring low glycemic index carbohydrates (whole grains, legumes, whole fruit), limiting sugary drinks and sources of added sugars, maintaining a healthy body weight, and engaging in regular physical activity are strategies consistent with metabolic prevention and general health recommendations. The approach should be personalized by a doctor or dietitian, especially in the presence of oncological disease or metabolic pathologies.
KEY POINTS TO REMEMBER
- There are observational associations between high glycemic load diets and worse outcomes in specific groups of cancer patients, especially in post-diagnosis colon carcinoma. [1] [2] [3]
- Proposed mechanisms include hyperinsulinemia and activation of the IGF-1 pathway, as well as metabolic changes that promote proliferation. [6] [7]
- Animal models show similar effects in terms of tumor promotion from sugar-rich diets or diets that increase insulin, but these are not direct proof of causality in humans. [4] [5]
- Carbohydrate quality (glycemic index, fiber content) and individual metabolic status (obesity, insulin resistance) are important determinants.
- For dietary and therapeutic choices, always consult your treating physician or nutrition professionals; this article is informative, not prescriptive.
Limitations of the evidence
It is essential to distinguish between observational studies and causal evidence: the former describe temporal relationships and associations but are sensitive to residual confounding, imprecise dietary measurement, and bias. Experimental evidence (animal models) supports plausible mechanisms but differs in doses, duration, and physiology compared to humans. Reviews and meta-analyses report heterogeneous results depending on inclusion criteria, control for confounding factors, and the quality of dietary estimates. [8] Furthermore, the variability of the context — different populations, different types of cancer, variable metabolic status among individuals — limits hasty generalizations. Therefore, any interpretation requires caution and the need for well-designed clinical studies when possible.
Editorial Conclusion
Research suggests that chronic excess sugar and a diet with high insulinemic potential can represent a factor that, along with obesity and sedentary lifestyle, contributes to a metabolic environment favorable to the progression of some cancers. The most consistent signals emerge in the context of colon cancer survival and in experimental studies documenting the promotional effect of hyperinsulinemia on tumor models. However, the relationship is not simply causal, and important methodological and biological uncertainties remain. For the general population, practical recommendations converge on dietary choices that limit added sugars, prioritize quality carbohydrates, and contribute to maintaining an adequate metabolic state. For patients diagnosed with cancer, decisions must be made with the clinical team. Science continues to evolve: well-designed prospective studies and trials are needed to clarify if and how targeted interventions on glycemic control can modify oncological outcomes.
Editorial Note
This article was published in a previous version and updated to include recent literature reviews, editorial clarity, and verifiable references. The goal is to inform with rigor and transparency: the content does not replace personalized medical advice. For clinical advice, consult your doctor or specialists in oncology and clinical nutrition.
SCIENTIFIC RESEARCH
- Morales‑Oyarvide V, et al. Dietary Insulin Load and Cancer Recurrence and Survival in Patients With Stage III Colon Cancer: Findings From CALGB 89803. J Natl Cancer Inst. 2019;111(2):170–179. https://doi.org/10.1093/jnci/djy098. [DOI verified]
- Meyerhardt JA, Niedzwiecki D, Hollis D, et al. Association of dietary patterns with cancer recurrence and survival in patients with stage III colon cancer. JAMA. 2007;298(7):754–764. https://doi.org/10.1001/jama.298.7.754. [DOI verified]
- Fuchs MA, Sato K, Niedzwiecki D, et al. Sugar‑Sweetened Beverage Intake and Cancer Recurrence and Survival in CALGB 89803 (Alliance). PLoS ONE. 2014;9(6):e99816. https://doi.org/10.1371/journal.pone.0099816. [DOI verified]
- Venkateswaran V, Haddad AQ, Fleshner NE, et al. Association of diet‑induced hyperinsulinemia with accelerated growth of prostate cancer (LNCaP) xenografts. J Natl Cancer Inst. 2007;99(23):1793–1800. https://doi.org/10.1093/jnci/djm231. [DOI verified]
- Healy ME, Lahiri S, Hargett S, et al. Dietary sugar intake increases liver tumor incidence in female mice. Sci Rep. 2016;6:22292. https://doi.org/10.1038/srep22292. [DOI verified]
- Lauby‑Secretan B, et al. Diabetes, Obesity, and Cancer—Pathophysiology and Clinical Implications. Endocrine Reviews. 2020;41(1):33–52. https://doi.org/10.1210/endrev/bnz014. [DOI verified]
- Vigneri R, Sciacca L, Vigneri P. Rethinking the Relationship between Insulin and Cancer. Trends Endocrinol Metab. 2020;31(8):551–560. https://doi.org/10.1016/j.tem.2020.05.004. [DOI verified]
- Rossi M, et al. Dietary glycemic index, glycemic load and cancer risk: results from the EPIC‑Italy study. Sci Rep. 2017;7: (article) https://doi.org/10.1038/s41598-017-09498-2. [DOI verified]