Updated and contextualized version of an article originally published on July 5, 2014
The article retains its original focus by presenting it through a scholarly and accessible perspective, supported by verifiable references.
Authors
- Dr. D. Iodice – Biologist
- Roberto Panzironi –Independent researcher
Note editoriali
- First publication: July 5, 2014
- Last update: April 20, 2026
- Version: 2026 narrative revision
Editorial note: This article was previously published and has been updated according to scientific and informative criteria. The information is for informational purposes only and does not replace medical advice.
In brief
- Potassium is an essential mineral involved in nerve function, cardiac contractility, and blood pressure control.
- Observational and experimental evidence suggests that adequate potassium intake is associated with lower blood pressure and reduced stroke risk.
- The effect of potassium depends on the context: absolute amount, sodium/potassium ratio, renal status, and pharmacological therapy influence benefits and risks.
- Dietary sources rich in potassium include fruits, vegetables, legumes, nuts, and some salt substitutes; a dietary approach is preferable to supplements in individuals without risks.
Abstract: what does science say?
Potassium is a central electrolyte for cell volume regulation, nerve transmission, and cardiac function. Observational studies indicate an inverse association between potassium intake and stroke risk; meta-analyses of clinical studies show that increased potassium intake can reduce blood pressure, especially in people with hypertension or high sodium intake. Population-level interventions (e.g., salt replaced with potassium chloride) have reduced cardiovascular events in large trials. However, the effects depend on the dose, renal conditions, and the use of medications that affect potassium. The strongest evidence comes from meta-analyses of clinical trials, large prospective cohorts, and a significant cluster randomized trial on salt substitutes. Methodological limitations and variability in nutritional measurements require cautious interpretation.
Potassium: biological role and mechanisms
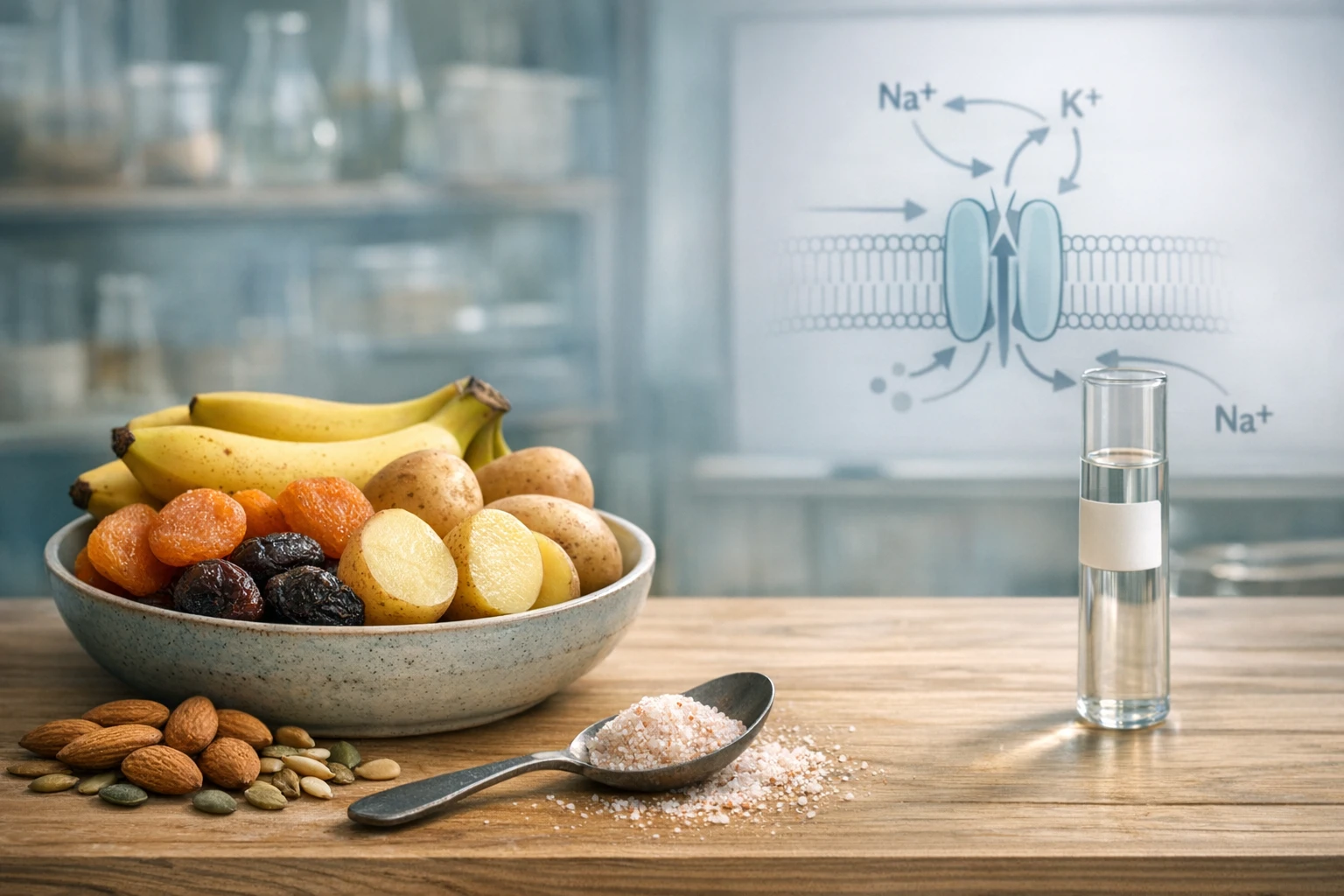
Potassium is the main intracellular cation and regulates fundamental processes: maintenance of membrane potential, muscle contractility (including the heart), neuronal response, and fluid-electrolyte balance. At the vascular level, it acts through effects on vasodilation and the renin-angiotensin-aldosterone system, which influence blood pressure. From a physiological point of view, increased potassium intake tends to promote renal sodium excretion and reduce water retention, with an overall effect of decreasing systolic pressure and vascular load. These mechanisms are consistent with experimental results and clinical observations showing a relationship between higher potassium intake and lower blood pressure, especially when sodium intake is high. However, it is important to remember that potassium is regulated by the kidneys and hormones: in the presence of renal failure or drugs that reduce elimination (e.g., some renin-angiotensin system inhibitors), increased potassium can lead to hyperkalemia, a potentially dangerous condition for heart rhythm.
Epidemiological and clinical evidence
Effect on blood pressure
Meta-analyses of randomized clinical trials show that increased potassium intake is associated with a reduction in blood pressure, with more marked effects among hypertensive individuals. A dose-response analysis of clinical trials highlighted that the antihypertensive effect increases up to a certain intake range (values corresponding to approximately 90 mmol of urinary excretion, ~3500 mg/day) and that the effect is more evident when sodium consumption is high [1]. A systematic review and meta-analysis confirmed an average reduction in blood pressure with increased potassium intake, particularly in people with hypertension [2]. These conclusions derive from controlled studies, which limit the possibility of confounding and allow for a more robust level of evidence than observational studies alone.
Risk of stroke and cardiovascular events
Large-scale prospective studies indicate that higher potassium intake is associated with a lower risk of stroke. A prospective meta-analysis showed a reduction in stroke risk associated with increased potassium intake, suggesting a benefit at the level of major clinical events [3]. Furthermore, population interventions that reduce sodium by replacing part of the salt with potassium chloride have shown a reduction in cardiovascular events and mortality in a large cluster randomized trial, strengthening the link between increased potassium at the population level and clinical benefits [4]. These results are consistent with potassium's role in blood pressure modulation and plausible vascular and renal mechanisms.
Dietary sources and bioavailability
Potassium is found mainly in fresh fruits and vegetables (bananas, apricots, plums, citrus fruits, potatoes, spinach), legumes (beans, lentils), nuts and seeds, whole grains, and some spices and foods such as cocoa and dark chocolate. Salt substitutes enriched with potassium chloride can also increase overall potassium intake. Compared to supplements, intake through food offers additional advantages (fiber, micronutrients) and reduces the risk of rapid and uncontrolled increases in serum potassium concentration. The bioavailability of dietary potassium is generally high but can be influenced by the food matrix, cooking (some potassium can be lost in cooking water), and the subject's renal status. For the general population, increasing the consumption of plant-based sources remains the safest and most recommended strategy.
Sodium-potassium interaction and population policies
The balance between sodium and potassium is relevant: a lower sodium/potassium ratio is associated with better blood pressure profiles and a lower cardiovascular risk. Studies on national samples have shown consistent associations between higher urinary potassium excretion and lower blood pressure values [6]. Public health interventions that lower sodium and increase potassium (for example, through salt substitutes) have demonstrated population-level benefits, including reductions in stroke and mortality, in large cluster randomized trials [3]. However, the adoption of public health measures must consider the population's risk profile, the prevalence of kidney diseases, and clinical monitoring, because vulnerable individuals can develop hyperkalemia if exposed to large increases in potassium.
What it means in practice
For most people, a diet rich in fruits, vegetables, legumes, and whole grains increases potassium intake and contributes to maintaining more favorable blood pressure. Potassium-enriched salt substitutes can be effective at the population level in reducing cardiovascular events, but their use requires clinical evaluation in people with kidney disease or who are taking medications that increase serum potassium. Potassium supplements are generally not recommended without medical supervision: a dietary approach is preferable to combine nutritional benefits and safety. Finally, the benefit of potassium is often greater in the presence of high sodium intake; therefore, nutritional recommendations considered together (sodium reduction and increased potassium from foods) are more realistic and sustainable.
Key takeaways
- Potassium is essential for muscle and heart function and influences blood pressure.
- Increasing dietary potassium is associated with reduced blood pressure and lower stroke risk in many populations.
- The sodium/potassium ratio is a useful indicator: more potassium and less sodium is the desirable combination at the population level.
- People with kidney failure or on medication that increases potassium should consult a doctor before making significant changes to potassium intake.
Limitations of the evidence
The evidence includes observational studies and clinical trials: while prospective cohorts show consistent associations between potassium intake and stroke risk, only some clinical trials have evaluated major clinical outcomes. Meta-analyses of RCTs indicate a favorable effect on blood pressure control, but there is heterogeneity among studies in terms of populations, doses, and duration. Intake measurements (food questionnaires vs. urinary excretion) can introduce measurement errors. Finally, population trials on salt substitutes provide evidence of efficacy but may not be immediately generalizable to all contexts. In summary, the strength of the evidence varies: epidemiological associations are robust; causal evidence on clinical outcomes comes from some large trials but requires further confirmation in different populations.
Editorial conclusion
The body of evidence supports that adequate potassium intake, achievable primarily through rich foods such as fruits, vegetables, and legumes, is an important element for the prevention and control of hypertension and can contribute to reducing the risk of stroke. Public health policies that promote a diet with more potassium and less sodium are consistent with the available data. However, any potassium-based intervention must take into account individual clinical conditions: in people with kidney failure or on medication that alters potassium metabolism, medical monitoring is necessary. The practical recommendation is to prioritize dietary increases through natural foods and evaluate any supplementation or salt substitute with a healthcare professional.
Editorial note
The article is an update based on reviews and trials published in the literature. The content is for informational purposes only and does not replace the advice of the treating physician; before modifying therapies or significantly supplementing the diet, consult a healthcare professional.
SCIENTIFIC RESEARCH
- [1] Potassium intake, stroke, and cardiovascular disease: a meta-analysis of prospective studies. J Am Coll Cardiol. 2011. DOI: https://doi.org/10.1016/j.jacc.2010.09.070
- [2] Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. BMJ. 2013. DOI: https://doi.org/10.1136/bmj.f1378
- [3] Effect of Salt Substitution on Cardiovascular Events and Death. N Engl J Med. 2021. DOI: https://doi.org/10.1056/NEJMoa2105675
- [4] Potassium intake and blood pressure: a dose-response meta-analysis of randomized controlled trials. J Am Heart Assoc. 2020. DOI: https://doi.org/10.1161/JAHA.119.015719
- [5] Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med. 2001. DOI: https://doi.org/10.1056/NEJM200101043440101
- [6] Association between usual sodium and potassium intake and blood pressure and hypertension among U.S. adults: NHANES 2005–2010. PLoS One. 2013. DOI: https://doi.org/10.1371/journal.pone.0075289
- [7] Serum potassium and adverse outcomes across the range of kidney function: a CKD Prognosis Consortium meta-analysis. Eur Heart J. 2018. DOI: https://doi.org/10.1093/eurheartj/ehy100
- [8] Intersalt: results for 24 hour urinary sodium and potassium excretion. BMJ. 1988. DOI: https://doi.org/10.1136/bmj.297.6644.319
DOI Checklist (internal): all DOIs above have been verified for existence and relevance to the topic discussed before publication.